
Parkinson's Patient care guide for Families
Complete Parkinson's home care guide for families, rehabilitation, safety and daily living.
Read MoreThis resource page aims to help family members, caregivers to support a loved one with Spinal Cord Injury. Discharging a family member after a spinal cord injury (SCI) brings many new responsibilities. This guide covers all major caregiving domains like prevent pressure ulcers, manage bladder/bowel, practice safe transfers, recognize autonomic dysreflexia (AD) and many more. If you need additional information please reach out to us. Our expert doctors will definitely help you with more specific inputs.
The spine is made up of small bones called vertebrae that protect the spinal cord - the body’s “main communication cable” carrying messages between the brain and the rest of the body. The spinal cord controls movement, feeling, breathing, bladder and bowel function, and many other body activities.
When a spinal cord injury happens, the effects depend on which level of the spinal cord is injured. This is called the neurological level of injury. In simple words, it means the lowest level in the body where movement and sensation are still working normally. Injuries higher in the spine usually affect more parts of the body.
The cervical spine is located in the neck. Injuries here are usually the most serious because they can affect both the arms and legs. A person may have weakness or paralysis in all four limbs, called tetraplegia or quadriplegia.
Higher cervical injuries (such as C1 - C4) may also affect breathing muscles, and some people may need ventilator support. Lower cervical injuries (C5 - C7) and C8 nerves may allow some arm and hand movement, helping the person become more independent in daily activities like feeding or wheelchair use.
The thoracic spine is in the chest and upper back area. Injuries here usually affect the trunk and legs, while arm function remains normal. This is called paraplegia.
People with thoracic injuries may have difficulty with balance, sitting posture, standing, or walking. Higher thoracic injuries can affect trunk control more severely, while lower thoracic injuries may allow better balance and sometimes assisted walking with braces or walkers.
The lumbar spine is located in the lower back. Injuries in this region mainly affect the hips and legs. Arm and hand function remain normal.
Depending on the exact level of injury, a person may be able to walk with support such as braces, crutches, or walkers. Bladder and bowel control may also be affected, and rehabilitation often focuses on improving mobility and independence.
The sacral region is the lowest part of the spinal cord, near the pelvis. Injuries here are generally less severe compared to higher-level injuries.
A person may still have some weakness in the legs, but walking is often possible. However, bladder, bowel, and sexual function can still be affected because these nerves help control those body functions.
SCI causes lost sensation and immobility, making pressure sores (ulcers) likely. Even a small red spot can become a deep wound if ignored. Untreated, pressure injuries may require months of healing, surgery or grafts.
Inspect skin every day (use a mirror or caregiver for back areas). Keep skin clean, dry, and well-moisturized (avoid excessive moisture). Shift weight every 15–30 minutes when in bed/chair: use wheelchair tilt or sit-up, or have a caregiver reposition you. Avoid dragging legs/skin across surfaces; lift rather than pull when sliding. Use linens without wrinkles and moisture-wicking fabrics. Drink adequate water as recommended by physician and eat well – dehydration and poor nutrition weaken skin.
Special foam, gel or air cushions and pressure-relief mattresses spread pressure. Examples: foam cushions (cheap, basic), air/ gel cushions (more pressure relief), alternating-pressure mattresses (pumps air in bed mattress to change pressure). See table below comparing options. Always use equipment as directed and get training on maintenance.
A new red, warm, hard or painful spot that doesn’t fade within 30–45 minutes is early (Stage I) pressure injury. Blisters, open sores or dark purple spots (Stage II–IV) demand urgent care. If redness persists or a sore appears, take pressure off immediately and call a doctor. Monitor any skin breaks daily; even small wounds need prompt treatment.
Pressure-redistribution is key. In bed: change position every 2 hours. In chair: do “weight shifts” by leaning side-to-side or using tilt/lean features every 15 minutes. Clean skin gently after any incontinence. Avoid hot baths or heating pads directly on skin. If a spot is noticed, do extra pressure shifts and keep area clean; seek medical care if it worsens.
The following video explains essential care tips for bedsores (pressure sores), focusing on safe cleaning and wound management. Learn why using normal saline is better than antiseptics for preventing infection and how to manage large wounds with loose dressing. Perfect for caregivers, nurses, and healthcare professionals, this guide highlights practical wound care techniques to improve healing, comfort, and patient recovery in everyday caregiving situations.
Equipment | Pros | Cons |
Foam/Wedge Cushions (basic) | Inexpensive, lightweight, easy to clean | Less pressure relief, may bottom out under weight |
Gel/ Fluid Cushions | Good pressure distribution, conforms to shape | Heavier, can leak/ puncture; often require maintenance |
Air Cushions | Excellent pressure relief; adjustable firmness | Expensive; risk of puncture, require frequent air-level checks |
Alternating-Air Mattress | Reduces pressure by cycling inflation; good for bed-bound | High cost, noise from pump, needs power/electricity |
Repositioning Schedule | Zero cost; effective if followed | Requires caregiver/time; fatigue risk |
SCI often causes loss of bladder control or emptying (neurogenic bladder). An automatic, regular schedule prevents urinary retention and infection. Caregiver knowledge of catheter care is vital.
Most use clean intermittent catheterization (CIC) every 4 - 6 hours. This means inserting a clean catheter to drain the bladder and then removing it. Other methods include an indwelling (Foley) catheter (left in place, drains to a bag) or suprapubic catheter (through the lower abdomen); external condom catheter for men (fits like a sheath). Your healthcare team will decide the best option.
Maintain a strict schedule: catheterize (or empty bag) regularly (e.g. 5 - 6 times/ day for IC). Wash hands before and after catheter use. Use one-time sterile catheters or thoroughly clean re-used ones. Keep catheter/ laundry and toileting areas clean. Empty drainage bags before they are half full, using separate toilet or flush outlet. Ensure tubing/ kinks aren’t pinching flow. Drink ample water (≥2 - 3 L/ day) to flush the system. Avoid holding urine too long – plan outings around accessible restrooms. Teach the person being cared for to signal bladder fullness if sensation is present. Record fluid in/ out.
SCI greatly increases UTI risk. Look for signs: cloudy, strong-smelling urine; fever, chills, nausea; new headache or increased muscle spasms; autonomic dysreflexia episode (for high injuries). Burning on catheter passage or abdomen/back discomfort may also occur. If any of these appear, consult a doctor promptly – UTIs can lead to sepsis. Prevention: always use clean technique, hydrate well, and consider cranberry juice or vitamin C to acidify urine. Encourage voiding on schedule to avoid overfilling.
Single-use sterile catheters latex/ silicon (lowest infection risk), hydrophilic (pre-lubricated) catheters (easy insertion, slick surface), if using indwelling catheters, inspect site daily. For men, a condom catheter is an option but must be sized correctly and changed daily to avoid skin breakdown. Consult your PM&R specialist and Urologist for the perfect bladder mangement.
Neurogenic bowel can cause constipation or incontinence. An individualized bowel program creates predictability and avoids complications like impaction and Autonomic Dysreflexia (AD).
Establish a routine (e.g. after breakfast or dinner). Maintain a high-fiber diet and plenty of fluids (at least 2 - 3 L/ day) to keep stool soft. Take prescribed stool softeners (docusate), fiber supplements, or laxatives at consistent times. Perform techniques: digital stimulation (gently insert gloved finger into rectum in circular motion) to trigger bowel reflex, and digital evacuation if stool is present. Enemas or mini-enemas or suppositories may be used. Empty one bowel movement per session (goal: within 30 - 60 min).
Keep notes: record each session’s outcome and any accidents.
Sitting upright on a toilet or commode enema bag can aid evacuation. If available, use a bowel-management stool that supports knees (kind of like a squat stance). Gently rubbing the abdomen in circles towards the rectum can help move stool along. Ensure privacy, warmth and a calm environment to relax the person (stress can inhibit bowel reflex).
Watch for hard, pellet-like stools or days with no bowel movement – these indicate constipation/ impaction. If impaction is suspected (no normal stool for 3+ days and overflow diarrhea), stop stimulants and use manual removal or doctor-assisted disimpaction as ordered. Bloating, cramps, or loss of appetite can also signal impaction. Incomplete emptying or incontinence should be discussed with the care team.
Note: bowel programs themselves (rectal stimulation) can trigger Autonomic Dysreflexia (AD), monitor blood pressure or have someone with you if injury is T6 or above.
Avoid constipating foods (bananas, cheese, white bread) and caffeine/alcohol which dehydrate. Gradually increase fiber and fluid if adjusting diet. Maintain mobility to aid digestion. Work with an occupational therapist on any special tools (e.g. digital stimulator devices).
Proper transfers and positioning maintain independence, prevent injuries, and protect skin/ limbs.
Perform daily range-of-motion (ROM) exercises (passive or assisted stretching of arms, legs, joints) to prevent contractures and spasticity. Change positions frequently in bed or chair: recline, side-lying, supine.
Always place cushions/pillows under heels and elbows to offload bony prominences. Keep the head of the bed slightly elevated to prevent sliding.
Use a gait belt or transfer belt around the waist when assisting with transfers.
Always: get close to the person, align hips/knees, keep your back straight, bend at knees, and lift with legs. Lock wheelchair brakes and bed brakes.
Remove armrests/ footrests as needed. Wear non-slip shoes on both of you. In case of a space/gap use a transfer board (bridging board) between surfaces. Pivot transfers: instruct the person to lean forward, then stand and pivot if they have leg strength. Slide-board transfer: have person slide across the board one hand at a time.
Keep living areas clutter-free; remove rugs or secure with non-slip backing. Ensure lighting is good. Install grab bars in hallways or near furniture to hold onto. Use assistive devices (walker, cane) only if recommended by a therapist. If the person begins to fall, guide them gently down (don’t attempt to catch full weight). Always have a plan to call for help (emergency button or phone in reach). Work with a physical therapist on safe transferring technique and any needed equipment.
Common mobility aids include: Manual Wheelchair (lower cost; self-propel if arm strength allows);
Prioritize what the person can do: if they have hand strength, encourage sliding; if not, use lift. See table below for a quick comparison.
Equipment | Uses | Pros | Cons |
Manual Wheelchair | Daily mobility | Lightweight, easier to transport, encourages active use of arms. | Requires upper body strength; may tire quickly. |
Power Wheelchair/ Scooter | Daily mobility | Electric drive, good for limited arm function or long distances. | Heavy, high cost, needs charging, less exercise. |
Transfer Board | Bed-chair, car-seat transfers | Simple, no tech, cheap. | Requires some upper body control; can pinch skin if not careful. |
Mechanical Lift (Hoyer) | Transfers when minimal strength | Safely lifts full weight; useful for caregivers. | Expensive, needs training, can frighten patient. |
Gait Belt | Assisted standing/transfers | Increases safety for both. | Must be fitted correctly (not too tight). |
Walker/ Cane | Partial walking aid (incomplete injury) | Helps stability, light. | Not for complete SCI, and risk of falls if misused. |
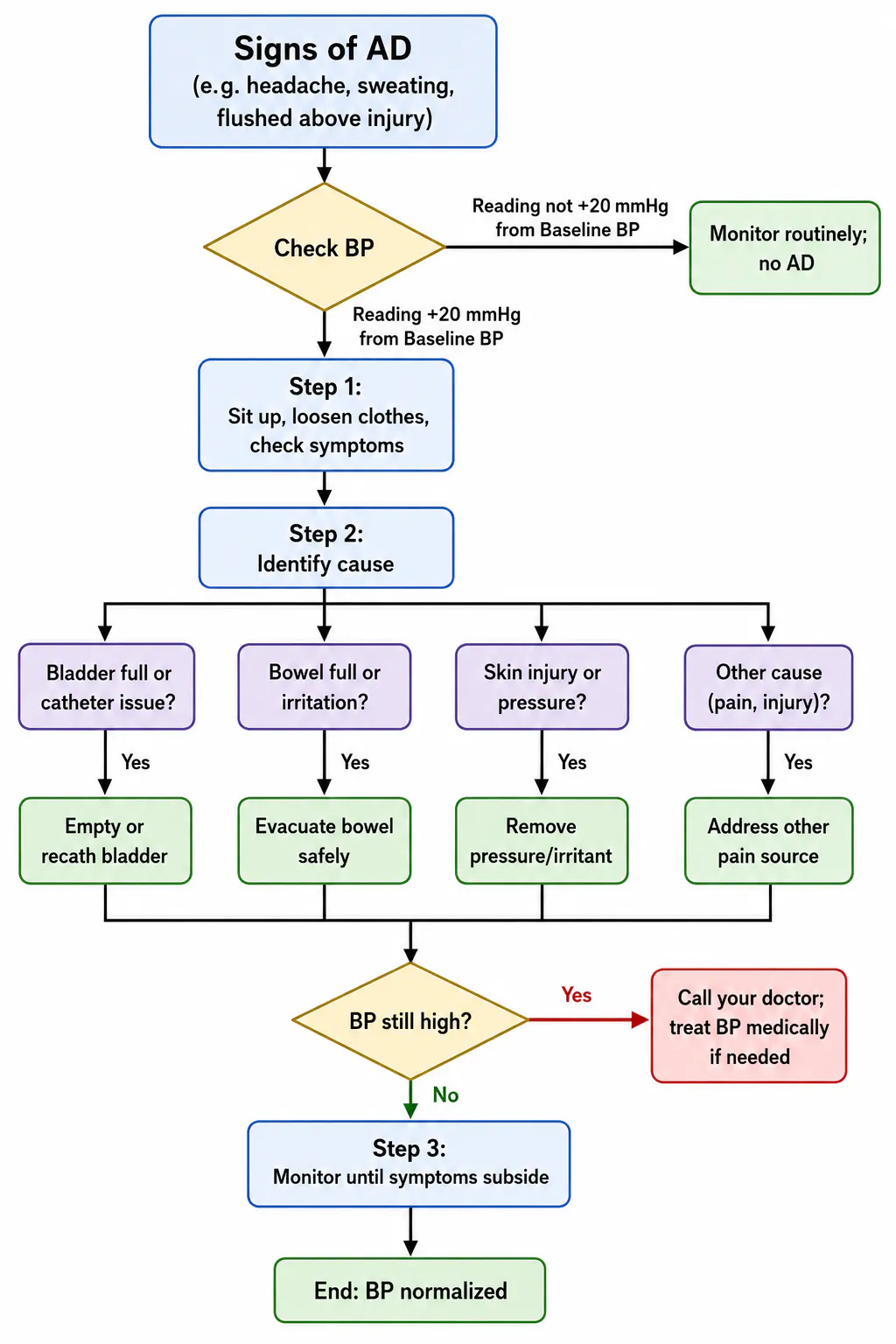
For injuries at T6 or above, pain or discomfort below the injury can trigger an uncontrolled surge in blood pressure. AD is life-threatening.
Most common is a full bladder or kinked catheter[39]. Also severe constipation, bowel impaction or hemorrhoids; tight clothing or pressure on skin (sores, ingrown nails); minor cuts/insect bites; or even blocked catheter tubing[39]. Sexual activity or menstrual cramps can also trigger AD.[39]
Sudden pounding headache, flushed or sweating skin above injury, goosebumps or “goose flesh”, and possibly nasal congestion or blurred vision[7]. Pulse may slow (rarely speed up). The person may feel anxious or uneasy. Take symptoms as an emergency. Check blood pressure if possible: AD is likely if systolic BP >150–160 mmHg (baseline could be lower).
Sit upright to lower BP. Loosen tight clothing (buttons, belts) and shoes. Call for help if caregiver is present.
Check for Causes: Quickly scan for triggers:
Call your doctor: You cannot find/stop the trigger, or symptoms/worsening BP continue. AD can lead to stroke or seizure. Notify emergency responders of “SCI with suspected AD” immediately (carry an AD medical card or list of usual triggers).
Prevention: Maintain consistent bladder and bowel programs; never skip catheterizations. Inspect skin daily and relieve pressure often (as above). Avoid tight clothing, straps or belts. Educate everyone in the home about AD signs and steps. Many caregivers keep a checklist (as above) at the bedside. Having a home blood-pressure monitor and nitroglycerin cream prescribed by a doctor can save critical minutes.
High-level SCI weakens breathing muscles (especially above C6), so lungs hold more secretions and infections (pneumonia) are common. Effective clearance of mucus and assisted breathing are critical.
Encourage the person to take deep breaths and cough several times a day. (Example: inhale deeply three times, then cough hard once on the third breath.) If unable to cough forcefully, caregivers can perform a “quad cough”: wrap arms around the person’s abdomen, time push outward during exhale. Only trained caregivers should do this. Use suction (mouth or trach) if the person has a tracheostomy.
Use an incentive spirometer as ordered: inhale slowly to raise a ball target to exercise lungs. A flutter valve or acapella device (handheld oscillation devices) can loosen mucus. Humidify air: steamy shower, humidifier, or drinking warm tea to thin secretions. Encourage activity or arm movement (like punching overhead) to expand lungs. Consider an abdominal binder to support diaphragmatic breathing.
If person has high tetraplegia (C1–C4), they may need assisted ventilation at night or always. Non-invasive support (CPAP/BiPAP machines with nasal mask) can help with apnea or weak breathing. Mouth or nasal suction machines and oxygen should be readily available if prescribed. For complete C1–C3 injuries, a ventilator (often via tracheostomy) is necessary. Work closely with a respiratory therapist for any breathing device; caregivers must be trained on use and alarms.
Watch for labored breathing, blue lips or nailbeds, or AD triggered by breathing effort. Fever or change in sputum may signal pneumonia; call doctor. If oxygen levels drop or person cannot breathe adequately (gasping, extreme fatigue), call emergency help. Keep up with annual flu and pneumonia vaccines.
SCI-related pain may be neuropathic (burning, tingling, stabbing below injury) or nociceptive (muscle/joint ache from overuse). Both need attention.
Establish a routine of stretching and positioning: gentle range-of-motion exercises for all limbs at least once a day. Apply heat packs to tight muscles or cold packs to inflamed joints. Massage contracted limbs if safe. Encourage relaxation techniques (deep breathing, meditation) to ease pain. Use supportive seating: cushions, back support, proper wheelchair posture. Educate patient to change positions frequently to relieve muscle tension.
If muscles stiffen or jerk involuntarily, help stretch the muscle slowly to reduce spasm reflex. Warm showers or Epsom salt baths can relax muscles. Remind patient (and self) that occasional spasms are normal; if they become very painful or frequent, note triggers (e.g. full bladder, pressure sore) and address those.
Use as prescribed by your Neurologist or Physiatrist (Physical Medicine & Rehabilitation). Schedule doses at times when rigidity is worst (often morning/evening). Keep heat/cold therapy, pillows, and a TENS unit available as non-drug aids.
Severe or new pain warrants medical review. Watch for triggers of AD hidden in pain (like tight spasm can itself trigger a headache). Maintain an open dialogue: chronic pain can cause depression, so ensure emotional support and professional pain management referrals if needed.
Good nutrition and fluids aid healing, skin integrity, and bowel/bladder function. After SCI, metabolism may slow (less muscle activity), so weight can creep up or down.
Aim for a balanced diet: high-quality protein (lean meats, dairy, legumes) to support healing; plenty of vegetables, fruits, and whole grains (fiber) for bowel health; and healthy fats (olive oil, nuts) rather than processed fatty meats or fried foods. Limit added sugars and simple carbs to prevent unhealthy weight gain. If weight loss is a concern (especially with high tetraplegia and low muscle mass), increase calorie intake with healthy options (nuts, protein shakes) after consulting a dietitian.
Consume 15–30 g of fiber daily and drink at least 2–3 liter of liquids (water is best). High fiber without fluid can worsen constipation, so adjust slowly and maintain hydration. Avoid excessive caffeine or alcohol (they can dehydrate and irritate bowel/bladder). Include fibrous foods (beans, whole grains) and prune juice to promote regularity.
Prepare balanced meals; involve the person in meal prep if safe (to encourage appetite and independence). Use adaptive utensils if needed. Plan snacks (nuts, cheese) to maintain energy between meals. For swallowing difficulties, adjust food texture (smoothies, ground meats). Consult a nutritionist for special diets (e.g. high-calorie formulas if person is underweight, or diabetic-friendly if needed).
Monitor for rapid weight change. Significant weight gain can make transfers harder and increase pressure sore risk; weight loss may indicate depression or medical issues. Keep a food log if needed. Report unintended weight changes to the doctor or dietitian.
It’s normal to feel shock, grief, anger or despair after SCI. Encourage open communication. Engage family in supportive dialogue.
Watch for persistent sadness, loss of interest, sleep/appetite changes >2 weeks. Depression is common (up to 1 in 4 post-SCI) but treatable. Provide emotional support and consider professional help (counselor, psychologist) early if symptoms appear. Encourage participation in support groups or peer mentoring programs (e.g. Christopher Reeve Foundation peer mentors).
Nightmares, flashbacks or anxiety attacks related to the injury event also occur. Reassure that therapy (trauma counseling, EMDR) can help. Create a calm environment at home; maintain routine to restore security.
SCI often changes sexual response: men may have erectile dysfunction and ejaculation issues; women may have altered lubrication or delayed orgasm. But intimacy and reproduction are still possible. Encourage open discussion about desires and fertility. Provide adaptive aids: erectile dysfunction medications (Viagra) for men, vibrators or vacuum devices for women. Address fertility: men may need sperm retrieval techniques; women can usually carry pregnancy (with obstetric monitoring). Discuss contraception and pregnancy plans with healthcare providers. Refer to a sexual health counselor or urologist/obstetrician knowledgeable about SCI. Normalize that intimacy may take new forms (e.g. gentle touch, novel positions, communication) to maintain closeness.
Recognize that caregivers also face stress. Watch for caregiver burnout (irritability, fatigue, sleep loss). Use the tips below and seek support (family, friends, caregiver groups).
Ensure step-free entry (ramp if there are stairs) and wide doorways (≥32 inches) for wheelchairs. Floors should be non-slip and clutter-free. Install lever-style door handles. Keep a clear path (≥36” wide) throughout main living areas. Place commonly used items (food, clothing, phone) at reachable heights (waist to shoulder level). Label switches and use voice-activated assistants if helpful.
Adjust bed height so feet touch floor when seated on edge. Use bed rails if needed. Place the bed in a corner for transfer support if needed. Ensure a clear turning space (5-ft circle). A hospital-style adjustable bed can assist with sitting up. Keep a commode chair near bed in case bathroom access is difficult at night.
Highest priority: install grab bars by toilet and in shower/tub. Fit a raised toilet seat or commode. Convert to a roll-in shower if possible, with a shower bench and handheld showerhead. Use non-skid mats. A transfer bench (extends from outside to inside shower) can help transfers. Consider a tub cut-out or remove the tub if wheelchair access is needed. Place towels, soap, etc. at reachable height. A hand-held shower and long-handled sponge aid those with limited arm reach.
Lower countertops or use a roll-under sink/ stove. Place cooking tools on wall hooks or shallow drawers. Use rocker switches or voice-activated appliances. Keep a sturdy chair nearby for seated food prep. Use adaptive utensils (built-up handles, plate guards) if self-feeding. Non-slip mats under cutting boards.
Arrange furniture to allow wheelchair turns. Secure throw rugs. Ensure reachable light switches (rockers) and electric outlets. Install pull-cords at reachable height for fans/lights. Keep telephones on bedside/table or use mobile/voice calling.
Identify two exit paths from each room. Keep hallways clear. Place emergency numbers and the person’s medical info (injury level, AD risk, medication list) on the refrigerator or by the phone. Have a small “go bag” ready with copies of IDs, keys, medications, catheters, and basic supplies. Test smoke detectors monthly and inform local fire department about the mobility needs.
Ramp, wheelchair, cushions, Hoyer lift, walker/ cane, shower bench, grab bars, hospital bed, floor lift (if needed), adaptive utensils, phone with speed dial. See table below for home adaptations.
Area | Adaptation Needed | Priority |
Floors | Remove rugs; secure carpets; no-slip flooring | High |
Bedroom | Adjustable bed; space to turn; bedside commode if needed | High |
Bathroom | Grab bars, shower chair/bench, roll-in shower or bath lift, raised toilet | High |
Kitchen | Lower counters/sink, grab bars, accessible storage, seated work areas | Medium |
Living Room | Wide paths (36″), reachable light switches, sturdy furniture at proper height | Medium |
Emergency | Emergency contacts list, medical alert/alarm system, smoke detector alerts | High |
Connect with other SCI families. Organizations like the Christopher & Dana Reeve Foundation offer peer mentoring programs and forums. Local SCI associations or rehabilitation centers often have support groups. Learning from someone who has lived with SCI builds confidence. (Contact an information specialist or nurse to find mentors.)
Encourage participation in adaptive activities (wheelchair sports, swimming, art groups). These improve mood and fitness. Many communities have adaptive swim classes, hand-cycle clubs or shooting sports. The caregiver can assist in finding and attending such programs.
Identify accessible transit options (paratransit services, wheelchair-accessible taxis) to enable community outings. Driving with hand-controls is possible in many states; check vocational rehab or DMV for modifications and training.
Plan regular outings (park, friends) to prevent isolation. Ensure venues are accessible and bring needed supplies (catheter kit, snacks, water). Use social media or local disability networks to find events.
If schooling is a factor, speak to school/ college disability services about accommodations (special seating, exam times). For children, involve school nurses and disability rights officers.
Many places offer grants for home modifications and equipment (e.g. VA Home Improvements and Structural Alterations for veterans). The first and most important step is obtaining a Disability Certificate and a UDID (Unique Disability ID) Card. Most schemes require a disability of 40% or more. Visit the UDID Portal for more information.
The UDID card serves as a national disability identity card and is increasingly mandatory for availing government disability benefits and schemes. It is valid across India.
Work with therapists to establish home-based rehab exercises (strengthening and ADL skills). Follow prescribed physical and occupational therapy schedules (often intensive at first, tapering to outpatient). Set realistic goals (e.g. improving transfer independence, arm strength) and track progress.
Vocational rehabilitation helps a person regain financial independence, confidence, social participation, and a sense of purpose after injury or illness. The goal is not just employment but finding meaningful work that matches the person's abilities, interests, education, and physical condition.
If returning to work or school is desired, apply for vocational rehabilitation services. State VR programs provide counseling and training at no cost. A VR counselor will assess interests/ skills, find suitable jobs or education, and help plan needed accommodations. Encourage use of “trial work” programs to test new jobs.
People with disabilities have the right to equal opportunities and protection from discrimination. Department of Empowerment of Persons with Disabilities has administers three Acts: under the Rights of Persons with Disabilities Act, 2016. Many employers are increasingly adopting inclusive workplace practices to support employees with disabilities.
Reasonable workplace accommodations may include adjustable desks, wheelchair-accessible workstations, computer adaptations such as voice-to-text software, accessible washrooms, private spaces for catheterization or medical needs, flexible working hours for therapy or medical appointments, and work-from-home options where feasible.
Often, simple modifications can make a significant difference. Adjusting desk height, providing ergonomic seating, improving workplace accessibility, modifying work schedules, or using assistive technology can help individuals perform their jobs effectively and independently. Open communication between the employee, rehabilitation team, and employer can help identify practical solutions that meet both workplace requirements and individual needs.
With appropriate accommodations and support, many people with spinal cord injury and other disabilities can successfully pursue careers in offices, educational institutions, businesses, government services, and remote work environments.
Use a pill organizer (weekly and four-times-per-day style) to sort medications. Attach a printed schedule of medications and dosages. Instruct any helper on each medication’s purpose.
Keep medicines in labeled containers, out of reach of children. For refrigeration-needed meds, ensure backup power or transfer in case of outages (e.g. insulin). Dispose of outdated meds.
Many SCI patients take numerous drugs (e.g. bladder meds, pain/spasm meds, blood thinners, etc.). Schedule them around routines (e.g. before/after catheterization). Use alarm reminders or apps. Always confirm with the care team when new meds are added or doses change.
Learn each medication’s side effects (e.g. some pain meds cause constipation; spasm meds cause drowsiness). If possible, have a pharmacist review all medications for interactions. If the patient has difficulty swallowing, ask for liquid forms or dissolvable tablets.
Practice good hygiene. Wash hands often, especially before/after catheterization or toileting. Encourage the patient to cough deep or use incentive spirometer after illness. Avoid crowds during flu season if possible.
As above in bladder section. Consider wearing gloves when handling urine if you are catheterizing frequently. Perineal care daily. Change absorbent garments (if used) immediately when soiled.
Change bed linens regularly. Treat minor cuts/scrapes immediately with cleaning and antibacterial ointment. Keep tetanus up to date.
Encourage vaccination (flu annually, pneumonia every 10 years. Keep humidifiers and ensure clean filters. Cover mouth when coughing. If chest infections occur, follow up quickly with antibiotics per doctor.
Position
Try to position the person on their side or slightly upright (30°) to aid breathing and reduce reflux. A foam wedge under the head or adjustable bed helps. Avoid lying flat for long periods if breathing is weak.
Bedding
Use soft, breathable sheets to prevent irritation. Check skin after sleep for any new redness or shear (especially if night-time transfers or shower cause friction).
Monitor for snoring or daytime drowsiness – sleep apnea is common post-SCI. If needed your doctor might recommend a sleep study and CPAP.
Maintain a regular bedtime routine. Fatigue can worsen spasticity and pain. Ensure patient gets enough sleep (8 hours adult, less for elderly if naps needed).
When to Call for Help:
Before discharge, learn all critical tasks from nurses/therapists: catheter insertion, skin checks, safe lifting, CPR, suction use, vent alarm management (if needed), etc. Take notes or video phone these training sessions if allowed. Ask what warning signs to watch at home.
Get a written discharge plan from the hospital, listing daily routines (B&B program, repositioning schedule, medications). Post it on fridge as a reminder.
Plan for occasional respite care. Use in-home aides or day programs so you can rest. Don’t wait until burnout – even a few hours a week can help mental health.
Keep regular communication with the rehab team (nurses, therapists). Use a health diary to log issues (skin spots, accidents, mood changes) and share at follow-ups. Use patient portals or call the clinic for minor questions.
Schedule follow-up appointments: usually first visit ~2–4 weeks post-discharge, then 3 months, 6 months, and annually (or as advised). Visits should include the rehab/SCI physician and specialists (urologist, orthopedist for any fractures). A full annual exam for bladder/kidney health is recommended (including renal ultrasound or urodynamics).
Continue outpatient physical and occupational therapy 2–3 times/week initially. Goals: regain as much independence as possible (e.g. self-wheelchair mobility, transfer alone, feed/dress themselves). Track achievements (e.g. “transfer to bed with one helper” or “sits unsupported for 5 min”). Adjust goals as progress is made.
These may include: returning to daily activities (showering, dressing), improving standing tolerance (if appropriate), pressure relief independence, or using adapted driving equipment. Document each goal and steps to reach it. Regularly re-evaluate and update with therapists.
Continue exercises prescribed by your rehabilitation team. These may include range-of-motion exercises, stretching, strengthening, balance training, standing practice, transfer training, wheelchair skills, or gait training (if appropriate).
Aim to gradually increase activity each day. Frequent short exercise sessions are often more effective than occasional long sessions. Follow the therapist's recommendations regarding standing frames, walkers, braces, wheelchairs, or other assistive devices.
For individuals with limited mobility, regular position changes, sitting out of bed, and pressure-relief techniques are essential to maintain circulation, lung function, skin health, and overall well-being.
Occupational therapy focuses on helping the person become as independent as possible in daily activities such as dressing, bathing, grooming, eating, toileting, and household tasks.
Adaptive equipment such as reachers, dressing aids, built-up utensils, shower chairs, or wheelchair modifications may improve independence. An Occupational Therapist can also recommend home modifications to improve safety and accessibility.
Practice everyday skills regularly and encourage the patient to perform tasks independently whenever safe. Small achievements build confidence and improve long-term function.
For individuals with cervical spinal cord injuries, improving arm and hand function is often a major rehabilitation goal.
Exercises may include grasp-and-release activities, picking up small objects, writing, using mobile phones, operating wheelchair controls, and performing self-care tasks. If muscle tightness or spasticity develops, regular stretching and consultation with the rehabilitation team are important. Splints or assistive devices may sometimes be recommended.
Maintain a binder or digital record of all therapy notes, doctor reports, and test results. This helps monitor improvement and is useful for future care decisions.
Knowledge That Guides Recovery
Get expert neuro rehabilitation tips from the doctors at Rehabana, Kolkata — simple guidance on stroke recovery, spinal cord injury rehab, Parkinson’s care, and enhancing quality of life after neurological conditions.
Complete Parkinson's home care guide for families, rehabilitation, safety and daily living.
Read More
SCI rehab guide for families after discharge. Skin care, mobility, bladder & bowel management, warning signs, recovery tips and safety steps.
Read More
Stroke rehab guide for families after discharge. Daily support, mobility, feeding, medicines, warning signs, recovery tips and safety steps.
Read More